As you fumble through the anesthesia drug tray, you begin to sweat. You notice that some drugs are missing. You quickly move to open the Pyxis machine but those drugs are missing, too. You swing open the heavy door to the operating room next door. Before you can speak through your mask, your colleague frames the question as a bewildered statement: “Let me guess, where’s the succinylcholine?”
Jerry A. Cohen, MD, past president of the American Society of Anesthesiologists (ASA), noted in 2012, “When I started practicing, I thought whatever drugs I needed would always be there. Now I open the drawer and occasionally something isn’t there.” In the past five years, according to the ASA, the United States has experienced shortages of an array of vital anesthetic drugs such as propofol, succinylcholine, even epinephrine.
The FDA began tracking drug shortages in 1999 in anticipation of possible manufacturing interruptions that might be caused by the Y2K computer scare. During the first year of the Drug Shortage Program (DSP), the FDA recorded shortages in the supplies of 61 different drugs. At that time, the shortages were caused by disruptions in regional distribution and often could be resolved locally.
Over time, however, the number of reported shortages has increased. By 2011, the DSP recorded shortages of 251 drugs, quadruple the number of drug shortages in 1999. And the drug shortages were no longer regional but national. Approximately 63% of shortages reported between January 2007 and June 2013 lasted an average of 340 days.
In response to the significant increase in drug shortages, the FDA required, rather than suggested, that pharmaceutical companies report all potential discontinuances of drugs used in the prevention or treatment of serious or life-threatening conditions. This included most anesthetic drugs.1
It appears the FDA’s actions have had some effect. Since implementation of mandatory reporting, the number of notifications to the FDA has risen sixfold. In response, the FDA has been able to prevent an increasing number of new national drug shortages (Figures 1 and 2).
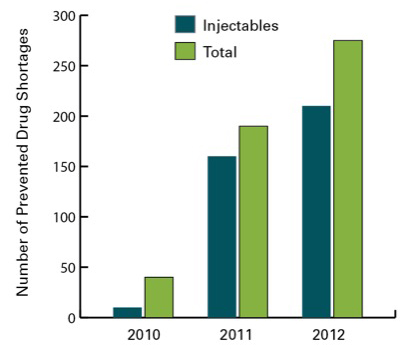
Figure 1. Number of drug shortages prevented by the FDA.
Source: FDA Internal Drug and Biologics Shortages Databases
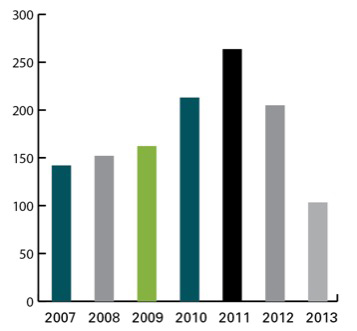
Figure 2. Number of new national drug shortages.
Source: University of Utah Information Service
Source: University of Utah Information Service
Even so, the number of active drug shortages has either remained steady since 2010 or has trended upward (Figure 3). In fact, 97.6% of anesthesiologists surveyed by the ASA in March 2012 reported experiencing a current shortage of at least one anesthetic drug. The anesthetic drugs most likely to be in short supply were fentanyl and neostigmine.
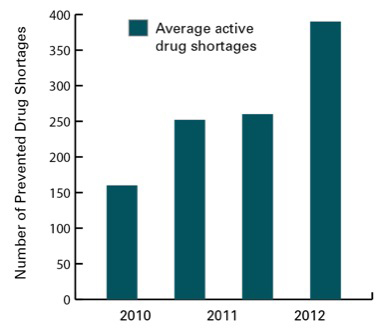
Figure 3. Average number of active drug shortages.
Source: University of Utah Drug Information Service
Source: University of Utah Drug Information Service

Figure 4. U.S. drug shortages by dosage form, July 3, 2014.
Source: FDA Drug Shortage Program
Generic injectable drugs are the most likely to be in short supply (Figure 4). These medications are 2.5 times more likely than brand-name injectable drugs to experience a shortage because approximately one-third of them are produced by only one or, at most, two manufacturers. In fact, only three manufacturers supply 71% of all generic injectable drugs.2-4
Because most injectable medications are used in the hospital and ambulatory care setting, it is not surprising that anesthesiology is among the specialties most affected by drug shortages. Propofol, for example, was the most frequently used anesthetic for outpatient surgeries in 2010, employed in nearly 70% of all procedures.5 Outside of the operating room, propofol is the most frequently used hypnotic in ICUs in the United States.6
All generic medications, not just generic injectable drugs, are more vulnerable to shortages than brand-name medications, in part, because brand-name medications usually have back-up manufacturing lines that provide redundancy in the event that one of the manufacturing lines goes down.2 Generic medications, probably because of their low profit margins, often are made on a single manufacturing line that also is being used to produce other products.7
Several important reasons exist for drug shortages. The first and most common (40% of shortages) is the issue of quality. Production lines may be contaminated with bacteria or particulate matter that necessitates closure of the production line. For example, in 2010, shortly after one manufacturer permanently discontinued production of propofol, a second manufacturer was affected by a quality problem that necessitated a temporary halt in production. The third and only remaining manufacturer of propofol simply was unable to meet the national demand for the drug.8
The second most common reason for drug shortages involves manufacturing delays caused by slowdowns and shutdowns for maintenance or remediation efforts (30%).4 Six of the top 10 manufacturers of sterile injectable drugs received warning letters from the FDA for serious violations of manufacturing standards between 2009 and 20129 which, in turn, required the manufacturers to address the concerns. The remediation efforts often require inspections, maintenance and equipment upgrades that either slow down or completely stop production of the drugs.
For most of the generic injectable products, there is only one manufacturer that produces the majority of a particular drug in the marketplace.2 Moreover, generic drug manufacturers are operating their production lines at full production capacity,4,10 24 hours a day, using equipment that is at least 50 years old, and using their manufacturing lines to produce not just one but multiple drug products.10 Thus, it is not uncommon for the manufacture of one drug to be halted because a second drug on the same production line has documented quality issues.
Only Getting Worse?
Looking to the future, the drug shortage problem may get even worse. In a review of 900 generic sterile injectable applications submitted to the FDA and approved between 2000 and 2011, only 1% of the applicants had a backup facility.10 Also, between 2006 and 2010 the number of generic sterile injectable drugs being manufactured increased by 52% without a commensurate increase in manufacturing capacity.4 The majority of the older facilities in the United States that already operate at full capacity will be manufacturing an increasing number of different types of injectable drugs on their production lines without any provisions for backup production if production lines are slowed or stopped.
Despite incremental steps that have been taken by the FDA, the agency does not have the authority to require a company to manufacture a drug, maintain certain levels of inventory or set drug prices. Manufacturers, therefore, do not have a strong financial incentive to upgrade their production facilities or aspire to exceed the minimum standards set forth by the FDA.2 In fact, the most common action taken by the FDA in 2011 was to ask other manufacturers to increase production.
Those manufacturers already running at maximum capacity and those who did not have the necessary equipment to increase production could not act on the FDA’s request. Also, many manufacturers maintain a “just-in-time” inventory and therefore do not have a supply of their drugs on hand to respond to any drug shortages.11,12 Nationally, companies have about two to three months of inventory on hand; wholesale distributors have about one month of inventory; and providers such as hospitals only have a few weeks of inventory. Despite the availability of public information regarding the precariousness of the drug supply in the United States, hospitals and other buyers have not responded to this information by holding larger inventories of drugs.
Anesthesiologists and their patients often are the victims of these drug shortages. In a summary of critical drug shortages reported between June 2011 and June 2013, anesthetic and central nervous system drugs were shown to have the highest frequency of critical shortages.10 The detrimental effects of these drug shortages for anesthesiologists include increased patient morbidity (hypotension, apnea, aspiration, prolonged mechanical ventilation, nausea and vomiting), longer anesthesia or recovery time, postponement of surgical procedures and even death.8,13-16
Succinylcholine, the most commonly used neuromuscular blocking agent (NMBA) for managing the airway in emergency situations,17 often is in short supply. Although anesthesiologists are the paragon of adaptability, alternative NMBA such as rocuronium may nonetheless result in life-threatening challenges in certain clinical situations. The use of a different NMBA in the absence of succinylcholine can lead to inferior intubation conditions,18 prolonged neuromuscular blockade, and an increased risk for difficulty ventilating and intubating critically ill patients.19
The adverse consequences of drug shortages are substantial. In a Premier Health report that surveyed 311 hospitals over a six-month period from July 2010 to December 2010, 89% of the hospitals reported drug shortages that caused a medication safety issue or error; 80% experienced a shortage that led to the delay or cancellation of care; and 98% reported a drug shortage that resulted in increased cost of care.2,20
Drug shortages also result in an increased number of “gray market” suppliers. These are suppliers who are not authorized by the manufacturer to sell the drug but, during a shortage, buy up the drug and resell it at inflated prices. Because these suppliers are not authorized by the manufacturer to buy or sell the drug, there is no assurance that the medications bought and sold in the gray market have been stored and transported properly.
Although progress has been made for the prevention of new drug shortages and to decrease the number of shortages, the FDA has room for improvement. Currently, no civil or monetary penalties exist for industry noncompliance.2,9 Despite a goal to collect data with the aim of predicting drug shortages, the FDA also has no way to internally authenticate the data’s validity. The collected data, according to a report from the U.S. Government Accountability Office, often relies on memories of events, email records and meeting notes without any mechanism in place to scrutinize and verify the information.1
Instead of waiting on the FDA to deliver further actions, anesthesiology and pharmacy departments could work together to mitigate and prevent shortages. One simple way involves improved communication regarding potential drug shortages as well as current drug shortages. This approach could mean designating a committee or members to drug shortages specifically. Often, anesthesiologists are not aware of a drug shortage until informed by the pharmacy department. As part of this communication, both departments could regularly check websites dedicated to drug shortages such as that of the FDA21 or the American Society of Health-System Pharmacists.22
If an alternative product must be used, educational material from the pharmacy could be sent out to the anesthesiology department to provide information on proper dosing limits, side effects, pharmacokinetics and other salient points. The pharmacy department in particular uses publicly available information about a manufacturer’s historical ability to provide quality products and reward companies who are more dependable. Relying solely on price is shortsighted.
With the above suggestions, perhaps you can help keep propofol, succinylcholine and epinephrine in your anesthesia trays.
No comments:
Post a Comment